THE POWERFUL DRUG AKA CHLOROQUINE
“It’s been around for a long time…and its very POWERFUL”
– POTUS
Current events
- Nature Article discussing in Chinese in-vitro research suggesting its use to treat COVID(1)
- Link
- 23 other ongoing clinical trials in China
- Link
- French Open label, nonrandomized clinical trial using combination therapy to treat COVID(2)
- People overdosing https://fox6now.com/2020/03/23/arizona-man-died-wife-critical-after-taking-fish-tank-cleaner-to-prevent-coronavirus-infection/
- People hoarding https://www.npr.org/sections/health-shots/2020/03/23/820228658/why-hoarding-of-hydroxychloroquine-needs-to-stop
Dosing
- The therapeutic, toxic and lethal doses of chloroquine are extremely close.
- A teaspoon of fish tank cleaner is potentially lethal. (4)
- 20mg/kg is a toxic dose
- Slightly more than one standard prescription for a 100kg person
- 40mg/kg without early intervention is a lethal dose
- Therapeutic dose
- Prophylaxis- 100mg daily or one dose of 300mg weekly for 6 weeks (1-2 weeks prior to exposure and 4 weeks after leaving an endemic area).
- Acute exacerbation- 600mg as the initial dose then 300 mg six hours later, followed by 300mg once a day for the next 2 days.
- No dosing recommendation for COVID-19 as not approved for off-label use yet.
- Possible Chloroquine dosing of 500mg PO BIDx1- days has been suggested. (5)
Mechanism of Action
- Mechanism of action- the drug inhibits synthesis of DNA and RNA thus it acts rapidly, and toxic manifestations appear rapidly, within 1-3 hours after ingestion
- Metabolism of this drug is very slow and as dosage increases the half-life increases.
Acute Toxicity
- In a retrospective study of 167 chloroquine poisonings the overall mortality was 8.4%(6)
- Cardiovascular Collapse
- Hypotension
- Primary effect is due to its membrane stabilizing action in the heart (quinidine-like).
- Induces negative inotropy which inhibits depolarization and decreases contractility and impaired conduction– effectively shuts down the heart.
- Hypotension
- Potassium Channel toxicity
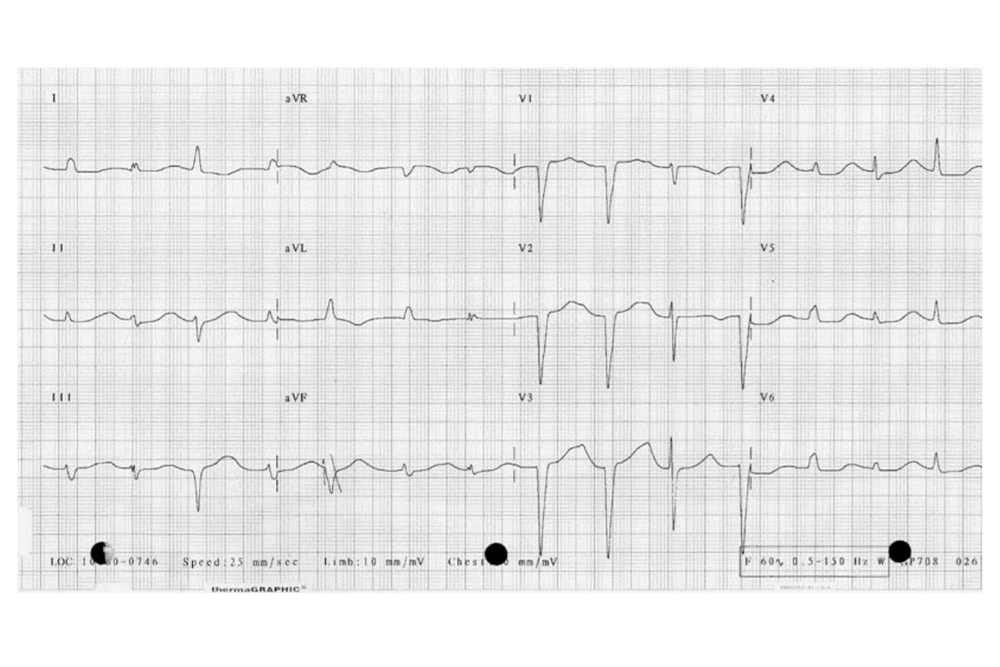
- Similar to TCA Overdose QTc- interval prolongation(7)
- Will lead to torsades de pointes
- Similar to TCA Overdose QTc- interval prolongation(7)
- Sodium Channel toxicity
- QRS widening >120 is the marker for increased mortality
- Will lead to Vfib/Vtach
- Hypokalemia can occur rapidly. Degree of hypokalemia appears to closely correlate with the severity of the ingestion.
- Seizures
Treatment
- GI decontamination with activated charcoal is recommended if ingestion in <1 hour.
- Cardiovascular collapse/Coma/Seizures
- ABC’s- Early intubation is important(8), Central line access early, Large doses of Epinephrine required and is the pressor of choice. (4)
- NEJM study in 1988 11 patients with an ingestion of 5g of chloroquine
- Better outcomes was with combination therapy of diazepam and epinephrine.(8)
- Diazepam
- Possible antagonist action against chloroquine toxicity possibly by having a direct cardiac effect.
- Use a loading dose of 2mg/kg (200mg for a 100kg individual!)
- Followed by continuous infusion (1-2mg/kg/day) for the next 24-48 hours.(8)
- Some studies however as with all things have also shown no benefit (at a significantly lower dose however) (6)
- Therefore OK to use other benzos in cases of shortage.
- QRS widening
- NaHCO3 (sodium bicarbonate)
- 1–2 mEq/kg boluses to obtain a serum pH of 7.45–7.55 or QRS <100
- infusion of 150 mEq mixed with 1 L of 5 % dextrose in water at a rate to maintain that pH.(9)
- Be careful with the bicarb administration and K+ replacement. Bicarb will lower potassium as well. (4) Can add potassium at 40meq/L.
- If between severe hypokalemia and QRS widening when weighing which treatment to prioritize, choose Bicarb.
- Consider hypertonic solution to avoid this scenario of necessary
- NaHCO3 (sodium bicarbonate)
- Hypokalemia
- Do not be afraid to give large infusions of potassium through a central line.
- Check potassium frequently; given there is no true potassium loss. As toxicity wanes, potassium will shift extracellularly and risk hyperkalemia.
Lab testing
- Monitor potassium levels
- every 4-5 hours during the first 48 hours after an acute toxic ingestion.(3)
- Glucose checks
- watch for hypoglycemia.(4)
- Serum chloroquine
- analysis is not readily available.(3)
Chronic Toxicity
- Ophthalmic Manifestations
- Rare complications
- Seizures, Auditory disturbances, neuromuscular excitability and/or coma may also occur.
Drug Information
- Chloroquine and hydroxychloroquine both in the quinolone class of drugs.
- Hydroxychloroquine is much less toxic (~40%) in animals.
- Chloroquine is highly effective as an antimalarial as well as an amebicidal agent.
- Hydroxychloroquine is used in autoimmune disease therapy such as Lupus, Rheumatoid arthritis.
- Chloroquine toxin has an affinity for melanin (pigmented) containing cells.
- Chloroquine and its active metabolite has been found in the pigmented ocular structures at concentrations much greater than in any other tissue in the body. It accumulates in the retina and continues to be retained long after its use is ceased.
References
- Liu J, Cao R, Xu M, Wang X, Zhang H, Hu H, et al.Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discovery. 2020;6(1):16.
- Gautret P. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an openlabel non-randomized clinical trial. International Journal of Antimicrobial Agents. 2020;In press.
- Scarfi C. Chloroquine. Clinical Toxicology Review. 2003;25(8).
- Chloroquine. American College of Meidcal Toxicology, 2020. Pheonix, Arizona.
- [Expert consensus on chloroquine phosphate for the treatment of novel coronavirus pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43(3):185-8.
- Clemessy JL, Angel G, Borron SW, Ndiaye M, Le Brun F, Julien H, et al.Therapeutic trial of diazepam versus placebo in acute chloroquine intoxications of moderate gravity. Intensive Care Medicine. 1996;22(12):1400-5.
- Holstege CP, Eldridge DL, Rowden AK. ECG manifestations: the poisoned patient. Emerg Med Clin North Am. 2006;24(1):159-77, vii.
- Riou B, Barriot P, Rimailho A, Baud FJ. Treatment of Severe Chloroquine Poisoning. New England Journal of Medicine. 1988;318(1):1-6.
- Bruccoleri RE, Burns MM. A Literature Review of the Use of Sodium Bicarbonate for the Treatment of QRS Widening. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2016;12(1):121-9
Article Peer Reviewed By:
Todd Phillips MD, FACEP @ToddToxTalks
Stefan Meyering DO, FAAEM @StefanMeyering



This Post Has 0 Comments