A 60 year old female presents to the ED with cc of chest pain and palpitations with associated shortness of breath for the past 3-4 hours. PMHx is significant for NIDDM, HTN, seasonal allergies, HLD. Pt takes singulair, atorvastatin, metformin, glyburide and cozaar. Denies inciting factors, other recent illness, travel or changes in medications. No hx of prior CAD, PE/DVT, dissection, prior ECHO/Cath/stress tests, hypercoagulable condition.
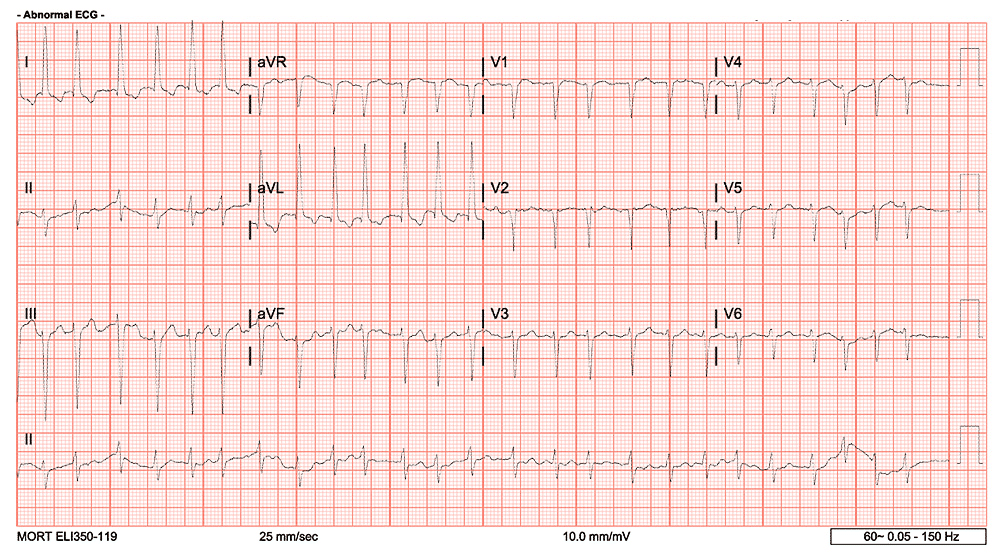
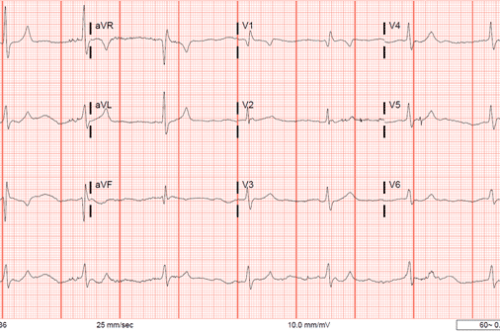
Initial EKG was obtained:
While this EKG does not show VT, and it appears to be somewhat irregular at points, it is relative difficult to say whether this is SVT with aberrancy, A-Fib with RVR, A-Flutter with RVR, or a re-entrant phenomenon such as AVNRT. certainly the rate is slower than typical for SVT/PSVT. The P waves are not readily discernable and are likely buried in the complexes however without directly viewing this determining the EKG finding here is more difficult.
Now, certainly we can trial some medications to uncover the rhythm – you likely would be well served with something like a CCB, BB or perhaps even adenosine in this particular patient, however if the patient was 20 instead of 60, something like procainamide or amiodarone would likely serve you better to avoid AV nodal blockade with underlying Antidromic AVNRT or WPW with aberrancy to help avoid precipitating a refractory rhythm ie VT/VF. However – Can we utilize the EKG to better uncover what the underlying rhythm is first?
The Lewis Lead
The Lewis lead configuration was described by Welsh Cardiologist Sir James Lewis (1881-1945) with the objective of enhancing P-wave amplitudes for better identification of atrial excitation in atrial fibrillation or flutter. He published this technique in a text in 1913 describing the lead placement to magnify atrial “oscillations” present during atrial fibrillation.(1,2,3)
So how do you perform the Lewis Lead EKG?
Start with a regular placement of precordial EKG leads – V1-6. Place the Right Arm (RA) lead over the manubrium. Place the Left Arm (LA) lead over the 5-6th intercostal space over the Right sternal margin, and place the Left Leg (LL) Lead over the Right costophrenic margin. The Right leg lead can stay on the right leg or be moved up into the RLQ of the abdomen. (2,3)
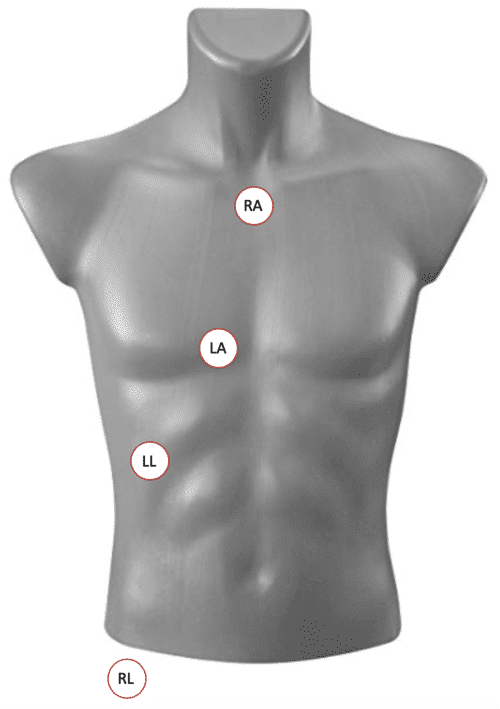
Image courtesy of TamingTheSRU – http://www.tamingthesru.com/blog/diagnostics/alternate-ekgs
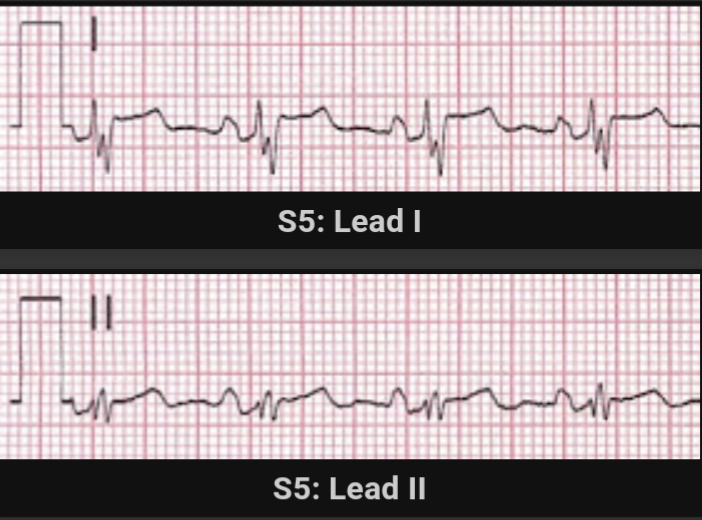
Now take a look at the EKG after performing the Lewis Lead placement.
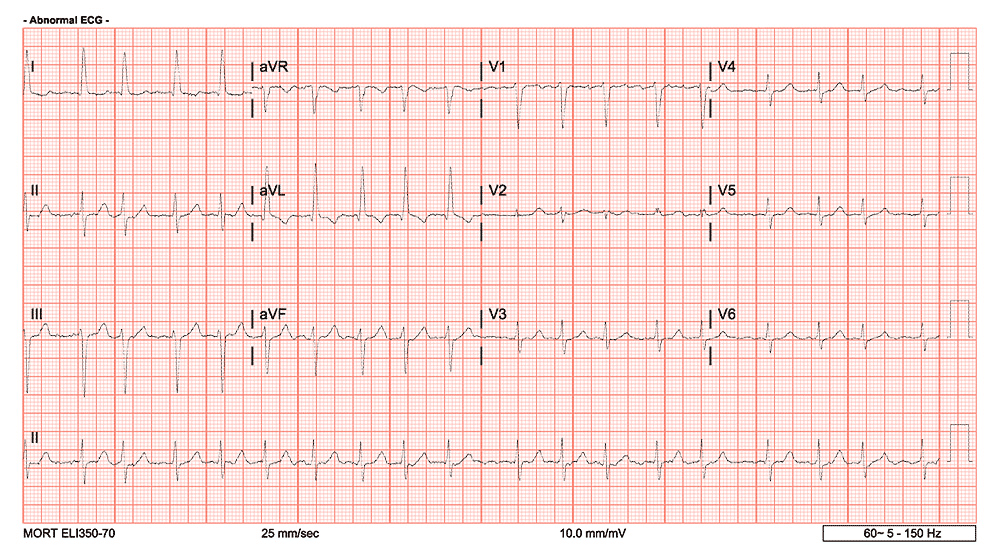
The rhythm has slowed down somewhat at this point however the P waves are certainly much more discernable here with the adjusted lead placement – leading us to uncover A-Fib with RVR as the rhythm, and effectively excluding something like SVT.
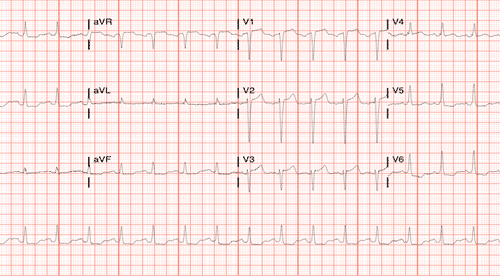
The patient was started on CCB infusion (diltiazem) and IV Heparin and the subsequent EKG was then obtained:
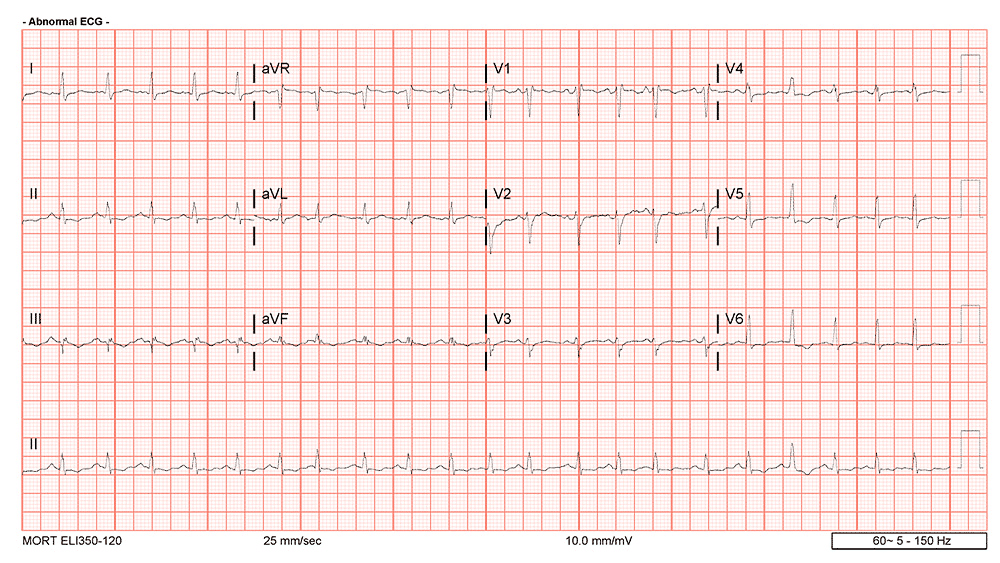
As you can see the patient has now converted to sinus rhythm, with readily discernable P waves.
This is a technique that can also be used for VT/Wide complex tachycardias and not simply just narrow complex rhythms. Because of their potential for causing hemodynamically compromise, a quick and reliable differentiation of the underlying rhythm is beneficial. Misdiagnosis of those tachycardias can often occur and lead to poorer outcomes.(4,5)
Here is another example of the application of the Lewis Lead arrangement to a wide complex tachycardia.
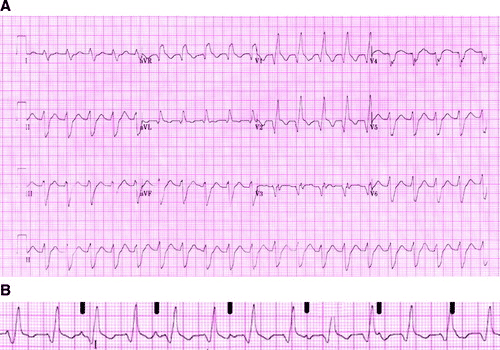
B is the Lewis Lead arrangment specifically for lead I
All credits of this image and EKG is courtesy of Circulation – https://www.ahajournals.org/doi/full/10.1161/circulationaha.109.852053
The original EKG is seen in A, whereas the Lewis Lead configuration has been applied and you are viewing lead I in B. The black markers denote the p waves present. You can see here that there is complete AV dissociation. In the setting of Wide complex tachycardia – this is NOT 3rd degree AV block – it is Ventricular Tachycardia.
A study in Clin. Cardiology in 2016 showed a sample of patients that had both regular and Lewis Lead EKG’s performed then interpreted by a cardiologist. The study showed that Ventriculo-atrial dissociation was present in 53% of ECGs in the modified Lewis-lead ECG group and 55% of ECGs in the standard-lead ECG group. This was correctly identified in significantly more patients in the modified Lewis-lead ECG group than in the standard-lead ECG group (mean, 71% vs 49%). The inter-rater agreement for correct detection of VA conduction type was moderate in both ECG groups, which emphasizes the difficulty of correct P-wave detection during VTs.
Overall this technique can help guide clinical evaluation and resuscitation measures. Make sure to test it out next time you have a patient with this type of presentation.
Image Credits
Stefan Meyering DO FAAEM – original images.
TamingTheSRU – http://www.tamingthesru.com/blog/diagnostics/alternate-ekgs
Circulation – https://www.ahajournals.org/doi/full/10.1161/circulationaha.109.852053
References
- Lewis T. Auricular fibrillation. In: Clinical Electrocardiography. 1913: 86-97
- Bakker AL et al. The Lewis lead: making recognition of P waves easy during wide QRS complex tachycardia. Circulation. 2009 Jun 23;119(24):e592-3
- Huemer M et al. The Lewis Lead for Detection of Ventriculoatrial Conduction Type. Clin. Cardiol. 2016; 39(2): 126–131
- Clin.Cardiol.39,2,126–131(2016) 131. Huemeretal:LewisleadforVA. Published online in Wiley Online Library(wileyonlinelibrary.com) DOI:10.1002/clc.22505 ©2016 WileyPeriodicals,Inc
- Stewart RB, Bardy GH, Greene HL. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med. 1986;104:766–771.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4463488/
- https://onlinelibrary.wiley.com/doi/pdf/10.1002/clc.22505
- https://www.ahajournals.org/doi/full/10.1161/circulationaha.109.852053
- http://hqmeded-ecg.blogspot.com/2018/03/hypotensive-and-tachycardic-in-clinic.html

This Post Has 0 Comments